


Understanding Tetracycline Stains on Teeth: Causes and Treatment Options
Tetracycline stains of teeth are a challenging dental concern that is caused by tetracycline antibiotics during critical periods of tooth development. These stains are not only aesthetically problematic, but may also be associated with compromised enamel integrity. Understanding their causes and exploring treatment options is crucial for effective management.
Causes of Tetracycline Stains
Tetracycline stains occur due to the unique interaction between tetracycline antibiotics and calcium ions during the formation of tooth enamel and dentin. Tetracycline and its derivatives have a strong ability to chelate calcium (Reference 1), leading to discoloration as the drug incorporates into the developing tooth structure. The degree and appearance of the staining vary based on several factors:
Timing of Antibiotic Administration:
The critical window for tetracycline-induced discoloration is during the calcification stages of teeth, typically from the second trimester of pregnancy to the age of eight. The earlier the exposure, the more pronounced the staining.
Duration of Use:
Prolonged use of tetracycline increases the likelihood and severity of discoloration. The longer the drug remains in the system during tooth development, the more it incorporates into the enamel and dentin.
Type of Tetracycline Derivative:
Different tetracycline derivatives, such as minocycline, may produce varying patterns and intensities of discoloration. Even fully developed teeth in adults can be affected by long-term ingestion of minocycline, leading to adult-onset staining. (Reference 2)
Genetic and Environmental Factors:
Individual susceptibility, such as genetic predisposition and dietary habits, can influence the severity of staining.
Characteristics of Tetracycline Stains:
Tetracycline stains present distinct patterns that make them identifiable:
Color:
The discoloration ranges from brownish-gray to yellow, with darker horizontal bands across the teeth.
Distribution:
The staining is often uniform but can vary in intensity across different teeth and regions of the enamel.
Enamel Quality:
In some cases, the enamel may also exhibit surface defects, cavities, or signs of wear, reflecting disturbances in normal amelogenesis during tetracycline exposure. (References 9 to 11)
Treatment Options:
Addressing tetracycline stains involves balancing aesthetic goals with preserving tooth structure and function. Treatment options range from conservative approaches like whitening to restorative interventions such as veneers and crowns.
1. Professional Dental Bleaching
Long-term professional bleaching can lighten tetracycline stains, but its effectiveness varies based on the severity of discoloration:
Vital Bleaching:
This involves using peroxide-based agents to oxidize and lighten stains over an extended period. While some patients achieve satisfactory results, this method may require months of treatment.
Limitations:
Bleaching may not uniformly address darker bands or deeply ingrained stains. It can also lead to dental sensitivity and a reduction in enamel hardness. (Reference 3 and 4)
Risks:
Prolonged exposure to bleaching agents has been linked to transient pulp irritation and potential toxicity to dental pulp cells. Caution and professional supervision are essential. References 5 to 7)
2. Microabrasion
Microabrasion involves the mechanical removal of superficial enamel layers using abrasive compounds and acids:
Effectiveness: This technique can improve the appearance of mild to moderate staining by removing surface discoloration.
Limitations: It is less effective for deep or widespread stains and may not address underlying enamel defects.
3. Dental Bonding
Bonding involves applying a tooth-colored composite resin to cover stains and improve aesthetics:
Advantages: This method is minimally invasive and can be completed in a single dental visit.
Limitations: Bonded restorations may discolor over time and require periodic maintenance.
4. Porcelain Veneers
Porcelain veneers are thin shells of ceramic material custom-designed to cover the front surface of teeth:
Effectiveness: Veneers provide a long-lasting solution for moderate to severe stains, offering excellent aesthetic outcomes.
Procedure: The process involves minimal enamel reduction and bonding the veneers to the teeth.
Durability: Veneers are resistant to staining and wear, but they require proper care and maintenance.
5. Dental Crowns
For teeth with extensive staining or structural damage, crowns can restore function and appearance:
Indications: Crowns are ideal for teeth with significant enamel defects, cavities, or wear.
Process: The tooth is reshaped to accommodate the crown, which is then cemented into place.
Benefits: Crowns provide comprehensive coverage and durability, effectively masking discoloration.
6. Combination Treatments
In many cases, a combination of treatments may be necessary to achieve optimal results:
Sequential Approach: For example, initial bleaching may be followed by veneers or bonding to address residual stains and structural concerns.
Customization: Treatment plans are tailored to each patient’s needs, considering the extent of staining, enamel quality, and aesthetic preferences.
Preventive Measures and Patient Education
While tetracycline stains are permanent once established, preventive measures can minimize their occurrence:
Avoidance During Pregnancy and Childhood: Tetracycline antibiotics should not be prescribed to pregnant women or children under eight to prevent developmental staining.
Alternatives: Healthcare providers can consider alternative antibiotics that do not affect tooth development.
Oral Hygiene: Maintaining good oral hygiene and regular dental visits can help manage surface discoloration and maintain overall dental health.
Conclusion
Tetracycline stains present a complex challenge that requires a thorough understanding of their causes, characteristics, and treatment options. While professional bleaching and conservative methods can address mild cases, restorative solutions like veneers and crowns offer more comprehensive results for severe staining. By combining advanced dental techniques with preventive measures, patients can achieve improved aesthetics and oral health despite the challenges posed by tetracycline stains.
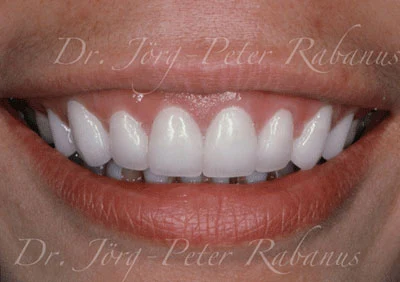
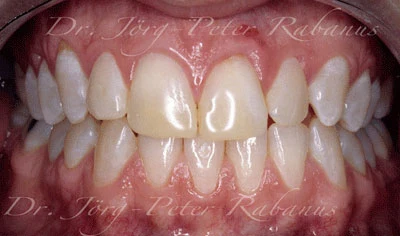
Examples of Smile Makeovers of Tetracycline-stained teeth:

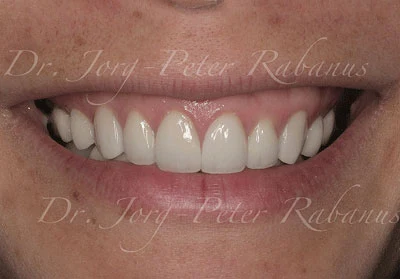
This Vietnamese patient had very dark teeth. She wanted naturally lighter teeth which could not have been achieved with a bleaching regimen. She received porcelain veneers.
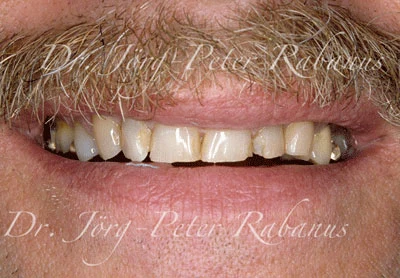
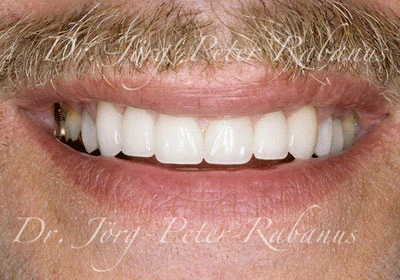
This patient had heavily worn and discolored teeth with large unsightly fillings. He requested to have his smile rejuvenated. Teeth were rebuilt to intact incisal edges and proper anatomical features. Proportions, forms, and balance were reestablished.
This patient came from Singapore for the treatment of her Tetracycline-stained teeth. She had already received some dental bonding in her country; obviously with only limited success. She received 10 upper veneers as seen on the picture on the right. One year later she decided to also cover her lower 10 front teeth with porcelain.

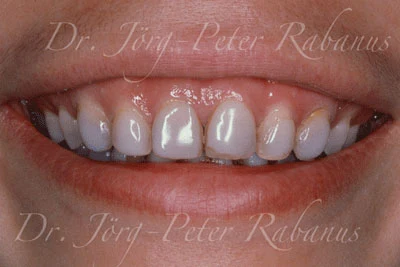
This patient had old and discolored direct composite restorations to replace missing tooth structure. They lost surface luster and their prior tooth color. The patient did not like the misalignment of her teeth, the spacing (diastemas) between the lateral incisors and the canines, and asymmetries at the gum line. Her concerns were addressed by performing a gum lift to create a symmetric gum line and porcelain veneers. The benefit of this cosmetic dental treatment approach is to address all concerns stated, dental misalignment, spacing, disproportionate tooth sizes, and dental discolorations. Meticulously bonded adhering to state-of-the art protocol and proper design to holistically integrate the new porcelain restorations into oral function, the patient will enjoy her new smile for many years to come.
References:
- Sanchez AR. Tetracycline and other tetracycline-derivative staining of the teeth and oral cavity. Int J Dermatol 2004; 43(10): 709-715.
- McKenna BE. Minocycline-induced staining of the adult permanent dentition: a review of the literature and report of a case. Dent Update 1999; 26(4): 160-162.
- Tsubura S. Clinical evaluation of three months' nightguard vital bleaching on tetracycline-stained teeth using Polanight 10% carbamide gel: 2-year follow-up study. Odontology. 2010; 98(2): 134-138.
- Eifallah HM. A review of the effect of vital teeth bleaching on the mechanical properties of tooth enamel. N Z Dent J. 2013; 109(3): 87-96.
- Auschill TM. Randomized clinical trial of the efficacy, tolerability, and long-term color stability of two bleaching techniques: 18-month follow-up. Quintessence Int. 2012; 43(8): 683-694.
- Lucier RN. Soft-tissue alterations following exposure to tooth-whitening agents. J Periodontol. 2013; 84(4): 513-519.
- Lima AF. Toxic effects of daily applications of 10% carbamide peroxide on odontoblast-like MDPC-23 cells. Acta Odontol Scand. 2013; 71(5): 1319-1325
- Ranggard L.Tetracycline as a marker in hard tissue research: effects on enamel formation in rat maxillary incisors. Scand J Dent Res. 1989; 97(5): 381-386.
- Westergaard J. Dose and age dependent variations in effect of tetracycline on enamel formation in rat. Scand J Dent Res. 1975; 83(1): 209-232.
- McIntosh HA. Tetracycline-induced tooth changes. Part 4: discoloration and hypoplasia induced by tetracycline analogues. Med J Aust. 1970; I: 114.
- Hilton HB. Tetracyclines in bones and teeth. Br Med J 1962; 2(5316): 1403.